
A word on lead placement and ECG filtering
Where the ECG leads are placed can change the view and sensitivity for detecting ischemia

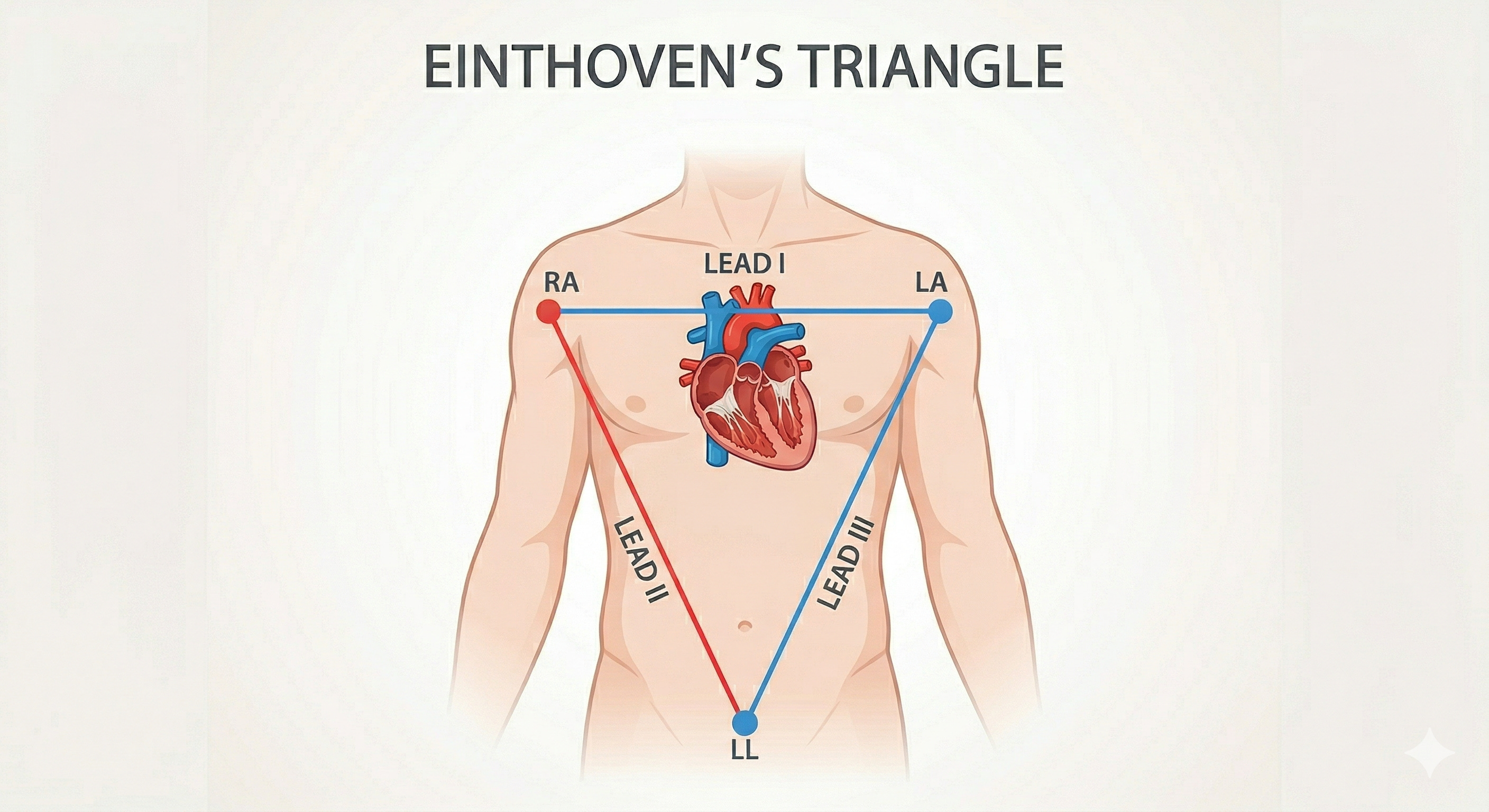
One of my pet peeves is finding a patient with the electrocardiogram (ECG) leads placed incorrectly. Correct positioning of the electrodes is paramount for accurate ECG interpretation.
Let’s look at the following example. Say the right upper extremity electrode (white, by the American Heart Association standards) is placed on the right shoulder, and the left lower extremity electrode (red) is placed on the left chest around the third intercostal space (I commonly see this sort of placement). Even if the monitor is displaying lead II, because of the electrode placement, what you will see will more closely reflect lead I.
The same applies to the precordial leads. If the electrode corresponding to the monitor’s V5 is placed on the sternum, you won’t be seeing lead V5. This sounds obvious, yet I see wildly misplaced leads every week.
Even misplaced leads will usually allow for accurate diagnosis of arrhythmias, but the sensitivity for detecting myocardial ischemia may be compromised. For example, loss of R wave progression in the precordial leads can indicate an acute myocardial infarction. However, if those leads are placed incorrectly, you may never get an accurate picture of the R waves and subsequent changes.
ECG filtering
Where the right lower extremity lead (green) goes also matters because this lead is used to help filter out electrical noise. If it is placed close to the right upper extremity lead, or too close to the site of electrocautery, the signal processing can be degraded.1
ECG filtering is a fascinating and complex subject. The monitors we routinely use in the operating room and for telemetry apply different filters than those used when recording a 12-lead ECG. This is the reason that one may see what appears to be ST-segment elevation on the monitor only to have it be absent on the 12-lead ECG. For more reading on ECG filtering, see here, here, and here.
Aside from breast and thoracic surgery, it is usually possible to have optimal lead placement. If the surgeon is operating on the abdomen, place the lower limb leads on the hips. For breast surgery, one can place the leads more distally on the arms even if an axillary dissection is being performed. To the surgeon, if you’re not cutting through the ribs, do you really need me to move the precordial leads?
The nuances of ECG lead placement can rapidly lead you down a deep rabbit hole. For example, interference in the form of pulse-tapping artifact, can occur when a lead is placed over an artery or too close to a fistula.
thank you
I can relate as someone who almost had their military career halted by poor lead placement. Interesting that you use V5. The brown lead on sets I commonly see only have a V on the brown lead. Most references I find use the V1 position.