
Ketamine can reduce delirium, but perhaps only at low doses

Delirium poses a real harm to patients, especially our elderly. Emergence delirium, in particular, can be dangerous to both patients and staff. For these reasons, there is a real need to try to prevent delirium.1 Unfortunately, all of our anesthetic agents can cause delirium.
Dexmedetomidine is the only drug that is clearly associated with a reduced risk of postoperative delirium.2 However, many patients cannot tolerate it due to bradycardia or hypotension. This is where ketamine, with its favorable hemodynamic profile, could be beneficial. Unfortunately, whether ketamine reduces delirium is less clear than the evidence supporting dexmedetomidine. Studies have shown mixed results, with some meta-analyses showing it reduces delirium and others showing it has no benefit. Notably, many of the studies included in these meta-analyses used higher doses of ketamine (≥ 0.5 mg/kg).
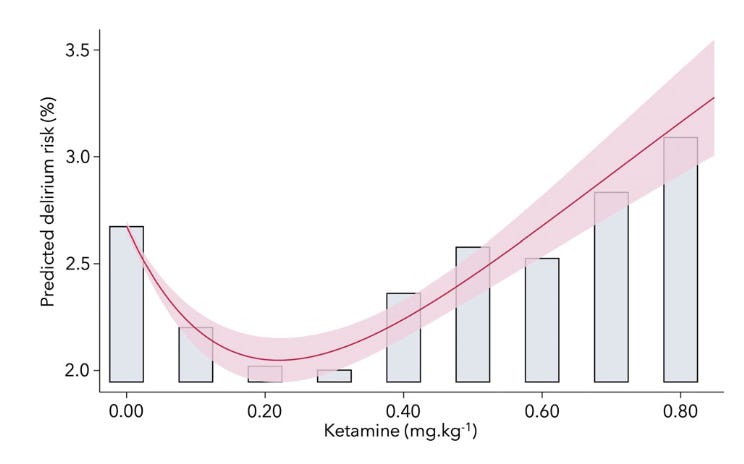
Several recent studies suggest using a lower dose of ketamine can reduce delirium. Let’s start with a retrospective study of 106,982 adults undergoing general anesthesia, which found that patients receiving ≤ 0.35 mg/kg ketamine had a lower risk of postoperative delirium compared to patients who either did not receive ketamine (adjusted odds ratio [aOR], 0.74; 95% confidence interval [CI], 0.59-0.89; p = 0.003) or who received > 0.35 mg/kg (aOR, 1.00; 95% CI, 0.85-1.18; p = 0.96). The incidence of delirium was 1.8% in the low-dose group, 3.1% in the high-dose group, and 2.7% among patients who did not receive ketamine. Modeling their data, the authors showed a U-shaped relationship between ketamine dosing and delirium, where both doses too low and too high failed to reduce delirium. They concluded that the optimal dose for delirium prevention was between 0.25 mg/kg and 0.34 mg/kg.
Now let’s look at the results of two recent randomized controlled trials (RCTs) that both compared 0.2 mg/kg of ketamine to placebo. In an RCT of pediatric patients undergoing adenotonsillectomy, the incidence of delirium in the ketamine group was 17% vs. 43% in the placebo group (relative risk, 0.40; 97.5% CI, 0.23-0.68; p < 0.001). In the second RCT, elderly patients undergoing arthroplasty under neuraxial anesthesia received either 0.2 mg/kg of ketamine intraoperatively and had ketamine added to a patient-controlled intravenous analgesia pump postoperatively, or they received placebo. The incidence of delirium in the ketamine group was 8.06% vs. 20.43% with placebo (aOR, 0.29; 95% CI, 0.14-0.63; p = 0.002).
These data suggest that the reason some prior meta-analyses have failed to show that ketamine prevents delirium could be due to higher dosing.
It would be great if we could entirely prevent postoperative delirium. Perhaps ultra-short-acting anesthetics, like remimazolam (which has some promising early data), could make a big difference. Until that time, low-dose ketamine could help reduce postoperative delirium in patients who cannot tolerate dexmedetomidine.
I am always skeptical of delirium research because I worry that it over-captures hyperactive delirium while missing hypoactive cases. Because the pharmacologic interventions targeting delirium are sedating, I also worry that we may simply be reducing the hyperactive symptoms while leaving patients still confused and now sedated.
For the remainder of this piece, I will use “delirium” to refer to postoperative delirium.