
New evidence suggests holding SGLT2 inhibitors prior to surgery may be harmful
SGLT2 inhibitor use reduced cardiovascular injury following cardiac surgery in a pilot study

A small pilot study caught my eye as it played into my biases about continuing sodium-glucose cotransporter 2 inhibitors (SGLT2i) in the perioperative setting. This retrospective study looked at adult patients on SGLT2i with left ventricular ejection fraction (LVEF) ≤ 50% who were undergoing non-emergent cardiopulmonary bypass (CPB). They were propensity matched with controls who were not taking SGLT2i, with each group containing 86 patients. Instead of being held for 3-4 days, patients in the SGLT2i group only had a dose held on the day of surgery.
The primary outcome was a composite of postoperative myocardial injury (defined as high-sensitivity troponin T > 70x the upper reference limit), low cardiac output syndrome (defined as requiring inotropes for > 48 hours or requiring mechanical circulatory support), and 30-day mortality. The composite primary endpoint occurred in 26.7% of subjects in the SGLT2i group compared with 41.9% in the matched controls (odds ratio [OR] 0.51; 95% confidence interval [CI], 0.27-0.96; p = 0.04). The primary outcome was largely driven by a reduction in myocardial injury, with 15.1% in the SGLT2i group compared with 41.9% in the control group (OR 0.46; 95% CI, 0.22-0.97; p = 0.04).
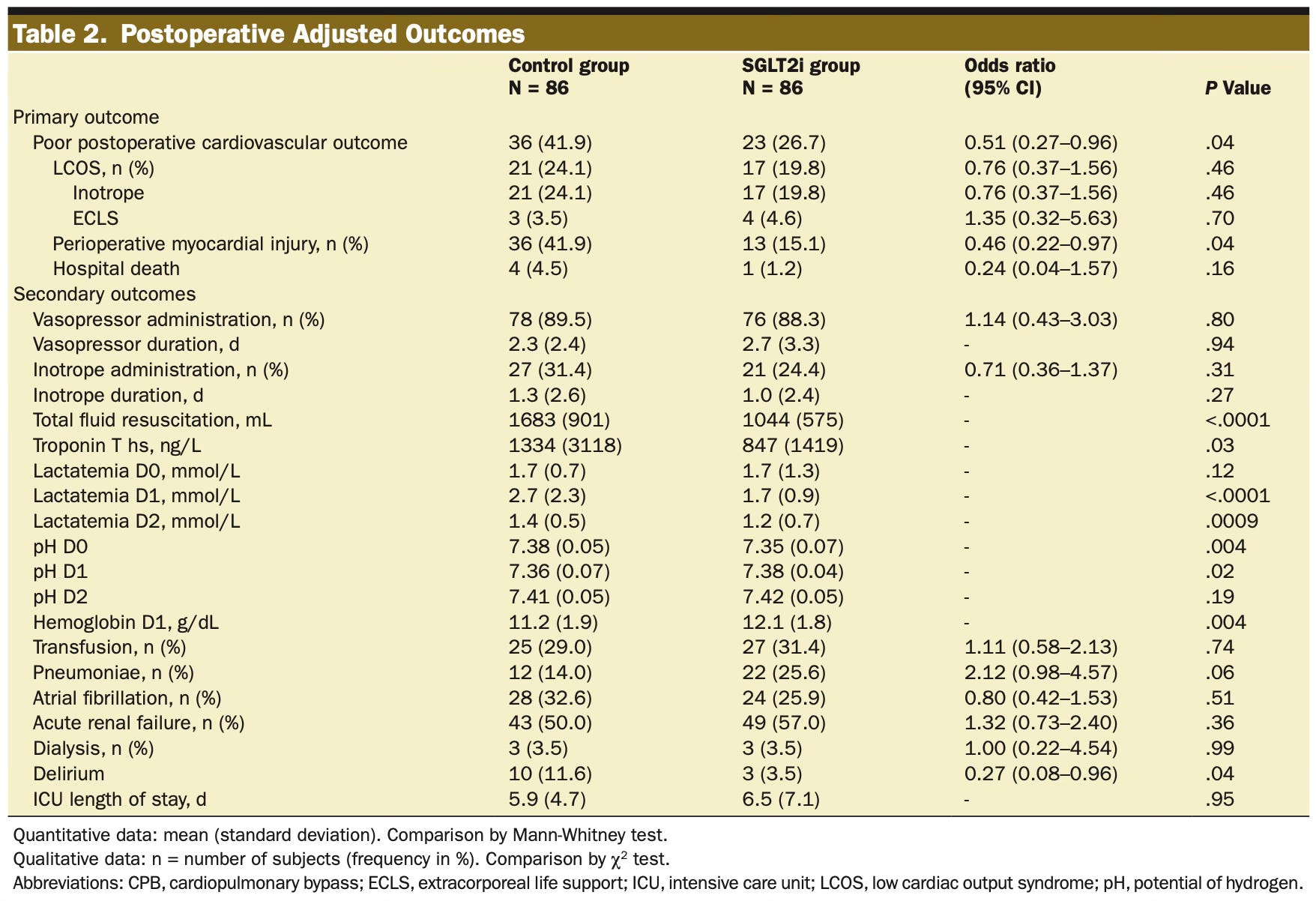
Before we conclude that SGLT2i should always be continued for surgery, let’s look at the limitations. The most significant limitations are the retrospective nature and relatively small sample size. The authors note that they did not have data on the incidence of ketoacidosis (diabetic or euglycemic), preventing us from weighing the potential risks of ketoacidosis1 against the benefits of protecting the myocardium. While the matching appeared to be well done, some differences in outcomes (listed in their Table 2) could have affected the results. Patients in the control group received approximately 60% more intravenous fluid than the SGLT2i group and had a nonsignificantly longer average time on CPB. Those in the SGLT2i group had a statistically significant shorter time to wean from CPB (20 vs. 25 minutes, p = 0.005).
The limitations should give us pause, but given the known cardioprotective benefits of SGLT2i, it is reasonable to think this acute cardioprotective effect is real. Hopefully, a randomized controlled trial also looking at the incidence of ketoacidosis (with measurement of preoperative and postoperative blood ketone levels) can confirm these results. Until that time, and considering the research showing no significant increase in diabetic ketoacidosis, these new data further suggest that the recommendation to hold SGLT2i for 3–4 days before surgery may be causing more harm than it is reducing.
If you want to dive deeper on topic, check out a recent podcast I did on ACCRAC discussing SGLT2 inhibitors and GLP-1 receptor agonists.
Because many hospitalized patients, and likely most ICU patients, receive insulin to tightly control their blood glucose, it is possible that the incidence of ketoacidosis would be lower due to the exogenous insulin suppressing ketogenesis. This could mean that the risk of ketoacidosis is much lower in an ICU population than in patients admitted to the floor.